

With so much evidence out there, it’s hard to know who or what to believe. For this reason, I’ve consolidated the most important points for you in this post to help navigate the minefield of information on shoulder pain and what you should really be doing about it.
I’m going to save you the trouble of reading the bulk of this article and let you skip to the bottom if you’re already convinced exercise is the way to go to help correct your shoulder pain but you need direction as to how.
BUT if you’re someone who is fed up with your should pain and is considering scans, surgery or injections, have a read through the following key points on each topic first and see if they don’t change your mind.
SCANS
-
Findings from radiology scans don’t definitively determine the cause of pain
Reports may find an ‘issue’ AND you may have pain but they may not be one and the same. The pain you experience isn’t necessarily coming from the findings from the report (10).
-
Scan results don’t tell you the cause of an injury
Diagnosis: Impingement. Rotator cuff tear. Subacromial bursitis.
Regardless of what a scan says, they cannot determine the underlying CAUSE of your injury
-
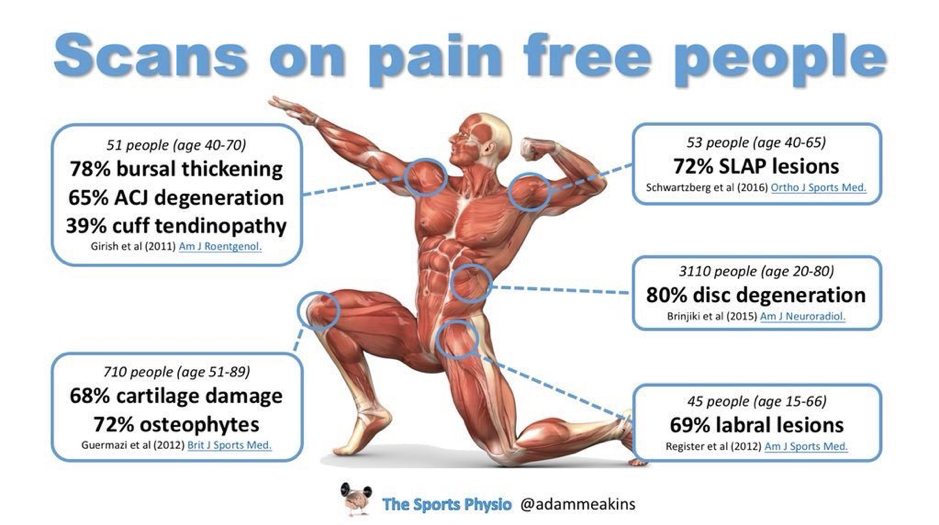
Up to 78% of PAIN FREE shoulders still have pathological changes on scans
This means you can have a scan diagnose you with structural ‘abnormal’ changes without you experiencing any pain at all (1). Equally, you may be in pain and have nothing show up on a scan.
SURGERY
-
Surgery provides similar results to exercise therapy
Going under the knife is a big deal. When there is evidence suggesting exercise provides the same benefits, if not more than surgical outcomes, it’s a no-brainer. The only caveat to this is with traumatic full thickness rotator cuff tears in which surgery is best (5).
STEROID INJECTIONS

-
Can provide good temporary relief
Pain relief and functional improvements have been noted consistently in the literature, however there are definite non-responders (people who find no benefit). Unfortunately, relief is short lived, lasting between 6-12 weeks (8).
-
Following injections, exercise therapy is recommended
This is not a one stop shop. Post injections, it is still recommended that you continue with exercise therapy. Similar outcomes have also been proven when comparing injection only with exercise only. Combination therapy may be beneficial (3,4).
EXERCISE
-
Improves strength, muscle tissue and stability

This should go without saying. Strength is one of the biggest determining factors to injury risk. The stronger and more stable your shoulders are, the greater their ability is to tolerate load and forces applied to them. The less ‘freak accidents’ occur.
FYI: It wasn’t reaching overhead or a single movement at the gym that caused your shoulder injury. It was the fact that your body wasn’t able to cope with the load, speed or repetitiveness of the movement you asked of it.
-
Treatment that actually addresses the cause
Anti-inflammatory medications, ice packs, heat cream, rest, surgery, injections and scans fail to do anything other than mask symptoms. Beyond removing pain, exercise is one of the only methods that has added benefits of being able to reduce re-injury risk (along with things such as nutrition, sleep and smoking cessation – all of which are within your control).
-
Promotes self-efficacy
Exercise is the only option here that you have control over. It is active, not passive. Someone else isn’t doing the work for you and while it’s nice to have a massage, to really fix issues you need to be in control of sorting the situation yourself (9). Find exercise professionals who can provide you with longer-term strategies and management tools to support and sustain strong, reliable shoulders for life.
-
Dopamine response post workout
The bonus ‘feel-good’ happy hormone high that you also get from eating chocolate.
So, what’s the definitive answer to solving your shoulder pain?
Best approach according to the experts and most up-to-date research
-
Start with a minimum 12 weeks of exercise-based therapy (4,11).
-
Avoid scans until after this time and only scan if issues are still present and no significant progress has been made after 12 weeks of exercise treatment (4,11).
-
Steroid injections are discouraged unless pain is so severe that it impacts your ability to perform your exercise rehabilitation. If you do get an injection, exercise is the recommended follow up treatment (4,11).
-
Surgery should be avoided. Exercise is equal to, if not better than surgical outcomes in most cases except in traumatic full thickness rotator cuff tears (5).
By now it should be pretty obvious exercise is best as a first line treatment. We also know avoiding movements that aggravate your shoulder won’t fix the underlying issue. Pain may subside with rest/avoidance, but the cause of pain is still there and pain is likely to resurface when you try to get back into exercising again. It’s a Catch 22.
You now know exercise is best to fix the pain, but you can’t exercise because of the pain.
Or maybe you can exercise, but you’re worried the pain you experience when you do is making it worse. Maybe you tried but it still isn’t fixed. Sound familiar?
When it comes to shoulder pain and exercise rehabilitation, there is no one size fits all approach. Which exercises are best and the needs of you as an individually need to be addressed based on your current capabilities, goals and requirements for the shoulder in question.
Are you a tradie who needs to use your shoulder and lift heavy, awkward objects everyday with goals to lift heavy and build muscle mass?
Do you work in an office and have to sit at a computer for 8+ hours and just want to lose a few kilos?
Are you an aspiring athlete who competes in a predominant upper body sport/activity and your next competition is fast approaching?
Tailoring exercise programs is my specialty. As an Exercise Physiologist I specialise in getting people out of pain and performing again.
If you would like further assistance with your shoulder pain but still aren’t sure if I’m the right person to assist, I offer complimentary calls HERE. If you’re ready to jump straight in, you can book both in person (Brisbane QLD Based) and Online Consults HERE NOW.
Brisbane based?
Next Saturday 18th January 2020 I am holding a FREE Workshop on Shoulder Health – from Pain to Performance. Link to tickets which must be secured before the day can be found HERE.
May your shoulders be strong and pain free!
Zenia Wood
Accredited Exercise Physiologist and Founder of Swift Movement Academy
—
P.S. For all my fellow nerd friends who want to read the research papers from this article!
REFERENES
-
Girish et al., (2011). Ultrasound of the shoulder: asymptomatic findings in men. AJR Am J Roentgenol. Oct;197(4):W713-9. doi: 10.2214/AJR.11.6971.
-
van der Windt, D A W M, & Bouter L. (2003). Physiotherapy or corticosteroid injection for shoulder pain? Ann Rheum Dis. May; 62(5): 385–387. doi: 10.1136/ard.62.5.385
-
Hay E M, Thomas E, Paterson S M, Dziedzic K & Croft P R. (2003). A pragmatic randomised controlled trial of local corticosteroid injection and physiotherapy for the treatment of new episodes of unilateral shoulder pain in primary care. Ann Rheum Dis. May; 62(5): 394–399. doi: 10.1136/ard.62.5.394
-
Maestroni L, Read P, Bishop C, Turner A. (2019) Strength and Power Training in Rehabilitation: Underpinning Principles and Practical Strategies to Return Athletes to High Performance. Sports Med. Sep 26. doi: 10.1007/s40279-019-01195-6. [Epub ahead of print]
-
Ketola et al (2013). No evidence of long-term benefits of arthroscopic acromioplasty in the treatment of shoulder impingement syndrome: Five-year results of a randomised controlled trial. Bone Joint Res. Jul 1;2(7):132-9. doi: 10.1302/2046-3758.27.2000163. Print 2013.
-
Hsu J, Keener JD. (2015). Natural History of Rotator Cuff Disease and Implications on Management. Oper Tech Orthop. 25(1):2–9. doi:10.1053/j.oto.2014.11.006
-
Karjalainen et al (2019). Subacromial decompression surgery for adults with shoulder pain: a systematic review with meta-analysis. Br J Sports Med Jan 15. pii: bjsports-2018-100486. doi: 10.1136/bjsports-2018-100486. [Epub ahead of print]
-
Cook T, Minns Lowe C, Maybury M, Lewis J S. (2018). Are corticosteroid injections more beneficial than anaesthetic injections alone in the management of rotator cuff-related shoulder pain? A systematic review. Br J Sports Med. Apr;52(8):497-504. doi: 10.1136/bjsports-2016-097444. Epub 2018 Jan 5.
-
Chester R, Khondoker M, Shepstone L, Lewis J and Jerosch-Herold C (2019) Self-efficacy and risk of persistent shoulder pain: results of a Classification and Regression Tree (CART) analysis. British Journal of Sports Medicine, pp.bjsports-2018-099450
-
Barreto R, Braman J, Ludewig P, Ribeiro L, Camargo P (2019) Bilateral magnetic resonance imaging findings in individuals with unilateral shoulder pain. J Shoulder Elb Surg, 1-8. doi:10.1016/j.jse.2019.04.001
-
Littlewood C, Bateman M, Connor C, Gibson, J., Horsley, I., Jaggi, A., … Scott, M. (2019). Physiotherapists’ recommendations for examination and treatment of rotator cuff related shoulder pain: A consensus exercise. Physiotherapy Practice and Research, 40(2), 87–94.












